COVID Treatment Options.com
Following is Zelenko's letter of March 23, 2020, copied to President Trump and Mark Meadows, that it would seem Google has effectively erased from the internet:
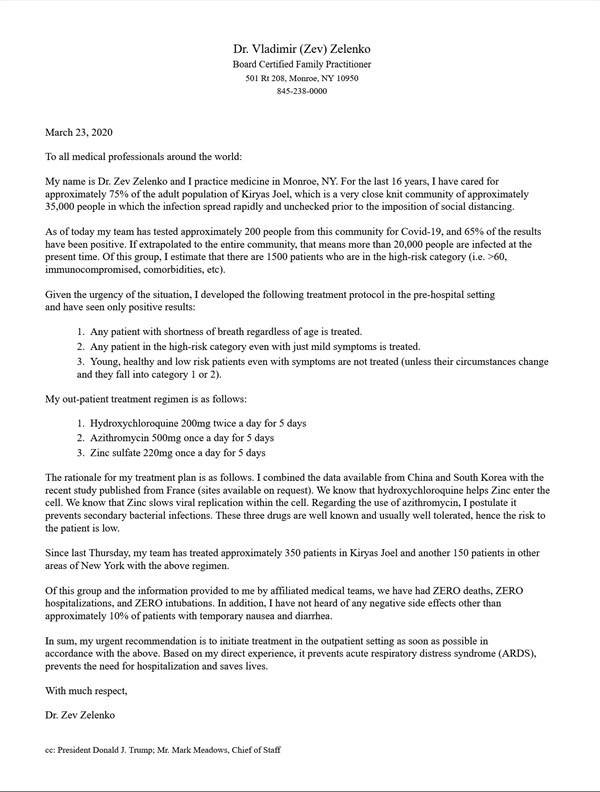
As time went on Zelenko expanded the treatment period to 7 days while including nutraceuticals like vitamins D, C and more. His team went on to treat over 7,000 COVID patients with only 4 deaths, one of which had stage 4 terminal leukemia while the other 3 sought treatment too late.
Over a million Americans died completely unnecessary, often horrific deaths, who could have otherwise gotten better in days at home through effective early treatment. However things would have been far worse if it hadn't been for thousands of talented, dedicated, collaborating clinicians, that met with near 100% success in treatment of their high-risk patients with $20 generic drug/nutraceutical protocols, employing a generic drug that enjoys a 65-year history as being one of the safest drugs on the planet.
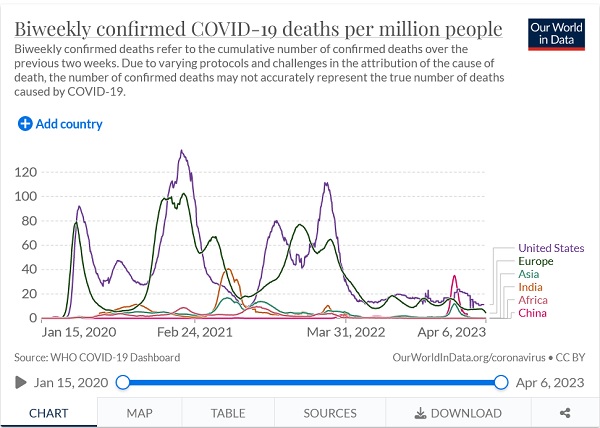
Did Big Pharma's also-captured Europe do much better?
Why didn't Anthony Fauci ever consult or collaborate with a single one of the thousands of front line treating physicians, that were enjoying success in treatment of up to 100% of their elderly and high-risk patients in the outpatient setting, when treated early upon presentation of symptoms or clinical suspicion of COVID-19? Where were the public service announcements to seek early treatment? Instead it was "go home and isolate" - in other words neglect yourself until you get sick enough to profit the illness industry - while treating your family and friends as if they were toxic waste.
The reason the blind eye was turned, is because if perfectly effective treatment with time tested safe generic drugs had been admitted to by our Big Pharma captured agencies, Emergency Use Authorization could not have been legally granted for patented, deadly, Remdesivir or the experimental, lethal, mRNA non-vaccines. And so the blizzard of industry, media and government profiteering lies and censorship began, buoyed up by compromised and outright fraudulent designed to-fail trials and studies. As Dr. Richard Horton, 20-year editor-in-chief of The Lancet once wrote: Journals have devolved into information-laundering operations for the pharmaceutical industry.
A peer reviewed retrospective study that demonstrated the 99+% success rate, for Zelenko's early treatment triple therapy protocol, is available on Science Direct at this link.
If all Americans had received Zelenko's level of care with a $20 generic drug triple therapy - immediately upon the presentation of symptoms or clinical suspicion of COVID-19 - the number of Americans that died of COVID over the first two years could have theoretically been 0, instead of a million. Even at an unrepresentative low 99% success rate, the two-year U.S. COVID death toll could have been about 10,000 instead of 1.2 million (flu deaths historically total about 30,000 to 50,000 annually). It is not possible to argue against the REALITY of successful early treatment through facts, data, science or evidence based medicine, as confirmed through practice by competent clinicians. All are welcome to try to refute the facts at this forum link. Send your best and brightest. TV white coats are more than welcome!
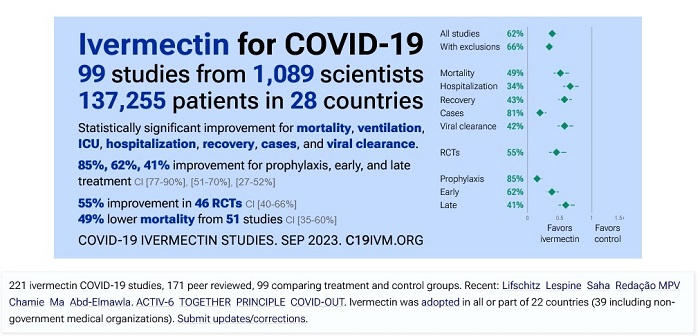
Another excellent therapy that came along in April of 2020 includes zinc + ivermectin + doxycycline (or azythromycin). The developers of ivermectin won the Nobel Prize in medicine for this, safe, cheap, 45-year-old off-patent generic drug, that has been prescribed for use in humans for over 35 years, with 3.5 billion doses having been consumed by humans to combat parasites like onchocerciasis (river blindness) and head lice as well as rosacea, scabies and more. It is safe enough to be administered in mass treatment, including when repurposed for COVID-19. Ivermectin may have an impressive 20 mechanisms of action against the SARS-CoV-2 virus.
Additionally, "Several studies reported antiviral effects of ivermectin on RNA viruses such as Zika, dengue, yellow fever, West Nile, Hendra, Newcastle, Venezuelan equine encephalitis, chikungunya, Semliki Forest, Sindbis, Avian influenza A, Porcine Reproductive and Respiratory Syndrome, Human immunodeficiency virus type 1, and severe acute respiratory syndrome coronavirus 2. Furthermore, there are some studies showing antiviral effects of ivermectin against DNA viruses such as Equine herpes type 1, BK polyomavirus, pseudorabies, porcine circovirus 2, and bovine herpesvirus 1."
Big Pharma's overt propaganda ministry, the FDA, characterized ivermectin as "horse paste" since for veterinary use it is administered to horses in paste form, yet they don't characterize aspirin as "horse paste", even though it is another therapeutic that is administered to horses in paste form.
MyFreeDoctor.com reported treating 150,000 COVID patients with only 4 deaths for a 99.99% success rate. Those 4 unnecessary deaths were among those that did not seek early treatment on a timely basis. If that had been the U.S. success rate from the beginning of the pandemic, our death toll over the first two years would theoretically have been just 27 instead of 1,000,000. Even at a poorly done 99% success rate there would have been only 5,000 COVID deaths per year instead of the over one million total.
Content on this free, clean, non-commercial website has been collected and reported on from world leading epidemiologists, virologists, microbiologists, pathologists, immunologists, vaccinologists, academics and particularly, talented, dedicated, highly successful front line treating physicians - the true scientists - regarding prevention and treatment of COVID-19. The embedded links on this page direct the reader to subjects covered in the forum. Meet a few of the world renowned medical professionals we rely on for forum information at this link.
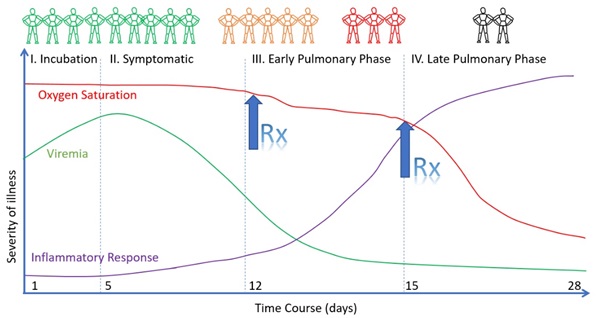
The exponential progression of the disease has been well known since early 2020. The longer treatment is delayed, the more complex the disease becomes, with the odds of an unfavorable outcome increasing exponentially.
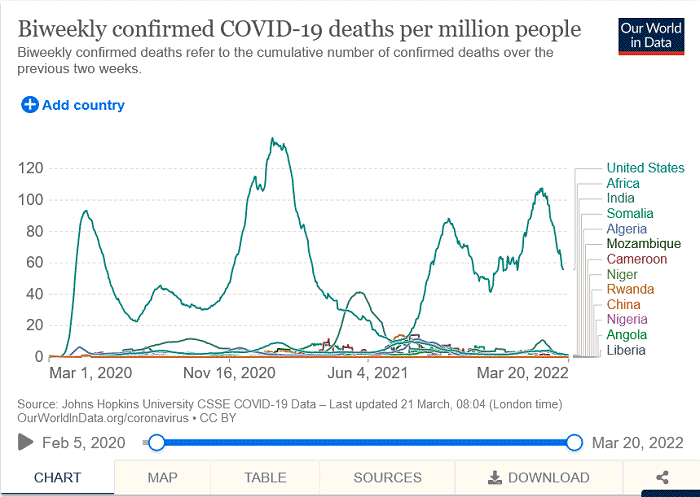
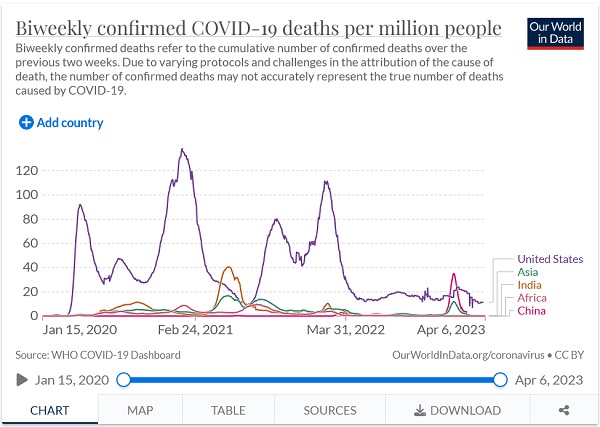
(link to here) Compare the U.S. COVID death rate where early treatment with IVM and HCQ have been suppressed, to that of impoverished, unsanitary, overcrowded 3rd world countries, where IVM and HCQ are as endemic as the parasites and malaria they treat.
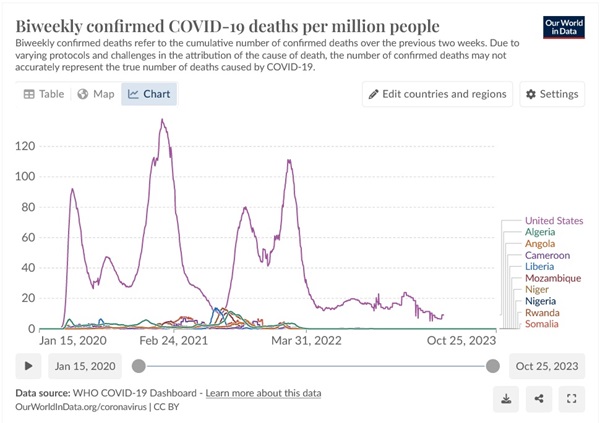
Some suggest that the reason that the U.S. has up to 400 times the COVID death rate of some African countries is because their population is on average younger. Is it reasonable to believe that could result in a 400 times lower death rate than the U.S.?
Let's compare U.S. with some African countries where they have effectively eradicated malaria, so the citizens don't regularly treat or prophylax for malaria with hydroxychloroquine. Selected from:
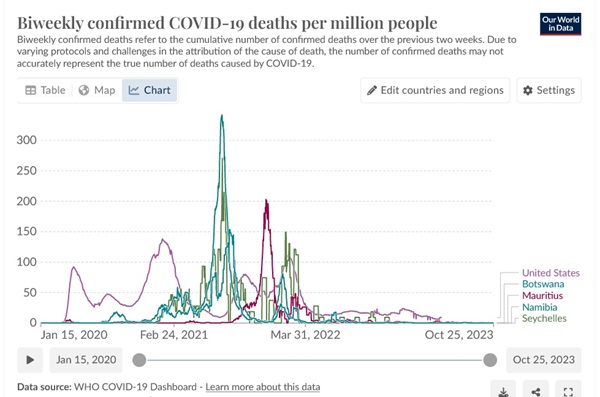
The Africa's "younger population" argument goes out the window. These low-hydroxychloroquine countries may be winning the battle against malaria, but they got nailed by COVID compared to their HCQ prophylaxed neighbors.
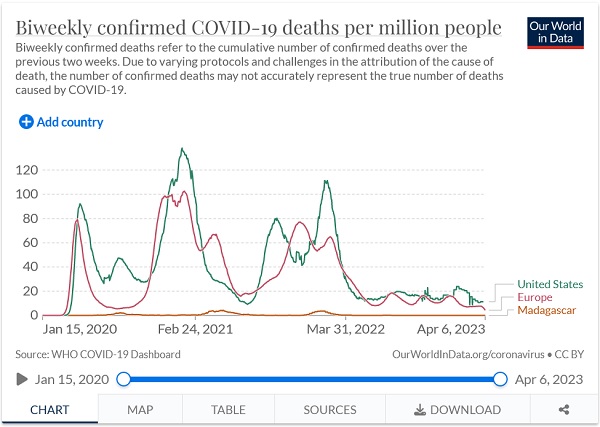
Compare the COVID death rate of Madascar, where sweet wormwood and ivermectin are popular, with the death rate in the U.S. and Europe:
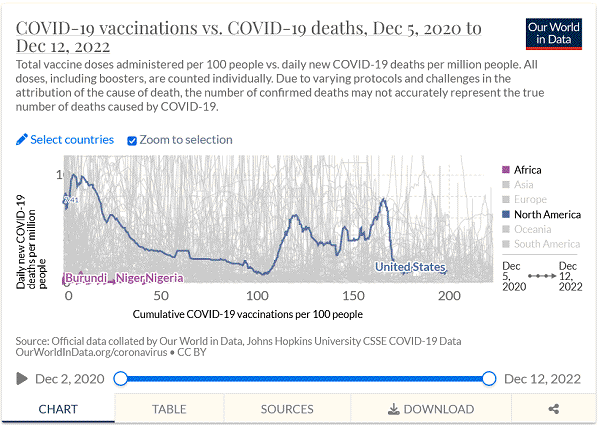
(link to here) Do these 10 African countries seem to have suffered from having had limited access to the experimental, leaky, rapidly waning, low efficacy, pathogenic priming, deadly, "vaccines"?
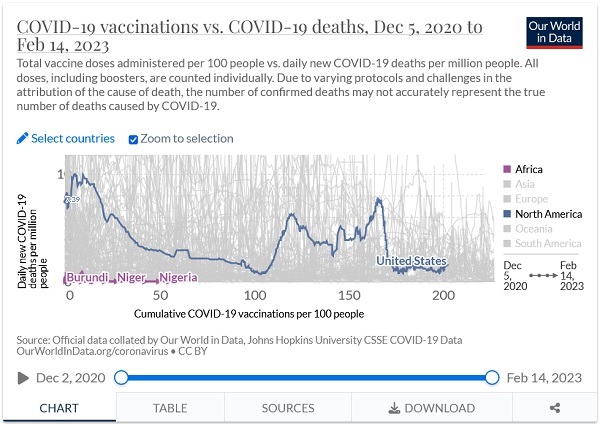
The reason that only Nigeria, Niger and Burundi labels appear in the above graph, is because the labels for Congo, Chad, Madagascar, Tanzania, Camaroon, Ethiopia and Mali, are underneath them. Those are W.H.O. numbers (example Nigeria).
Could Madagascar's low death rate be because they had such a high vaxx rate compared to the U.S.?
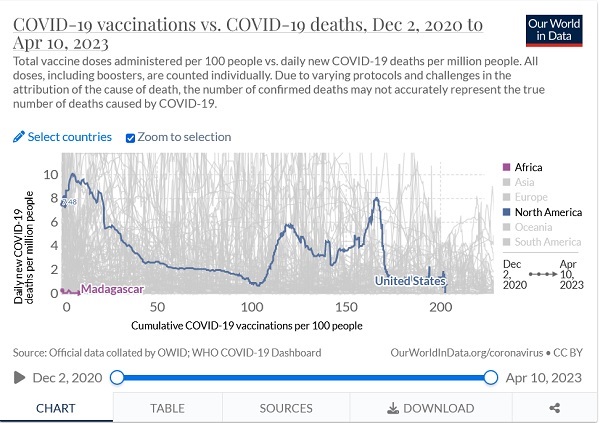
Obviously not.
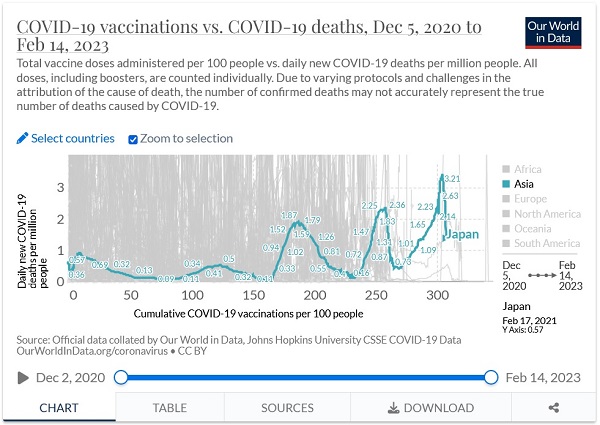
What does the following graph suggest about COVID vaxxing in Japan?
What "coincidence" does the shot appear to be effective at producing?
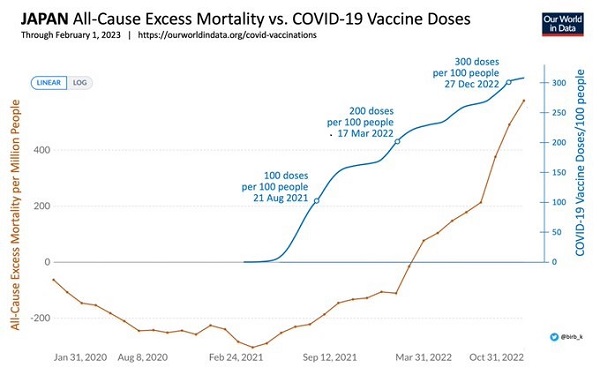
Did the "vaccines" ultimately reduce the COVID death rate in Japan?
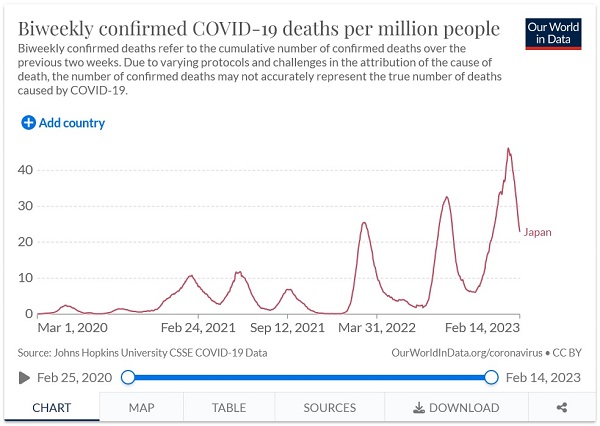
(link to here) Averaging three vaccines per person, Japan's COVID death rate increased to new highs, in each of 3 consecutive waves, as cumulative vaccine uptake increased.
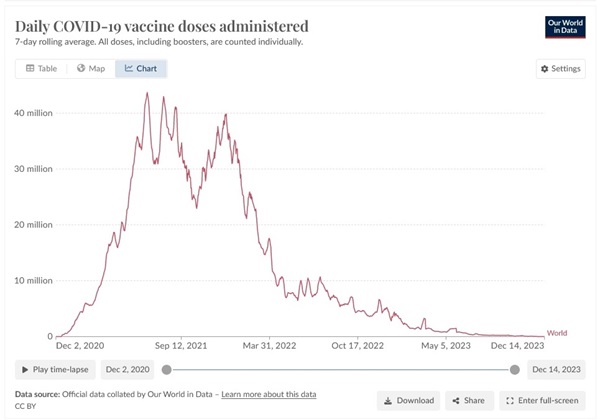
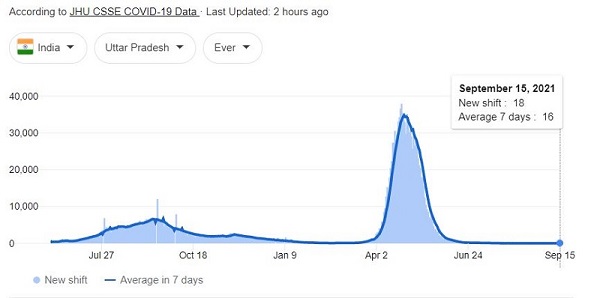
India smoothed along just fine in 2020, then along came the vaccine rollout:
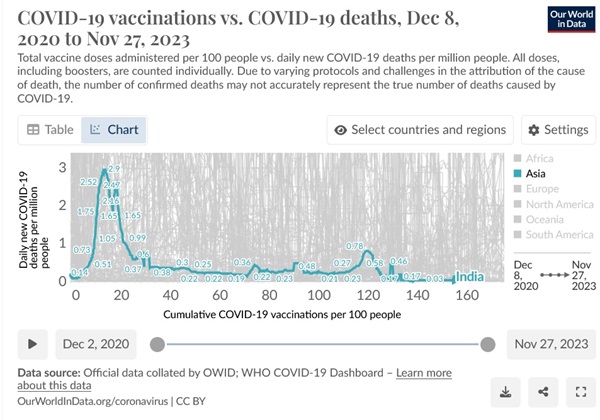
No surprise since a very large Cleveland Clinic study revealed that the more COVID vaccine doses a person receives the more likely they are to get COVID.
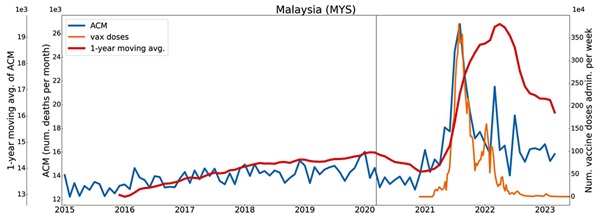
(link to here) Denis Rancourt (substack) (also of "Correlation") matched up the timing of all-cause mortality by the timing of the number of vaccine doses to arrive at the "vaccine dose fatality rate" or vDFR. A near perfect match in Malaysia is shown in the following graph. Is it reasonable to suggest the correlation demonstrates the causation?
By his preliminary calculations, 17 million people have been killed by COVID vaccines worldwide.
Is death or permanent disability what anyone wants for their children, considering a Johns Hopkins Study Found Zero COVID Deaths Among 48,000 Healthy Kids? Let alone the known risk of myocarditis to their hearts? As well as a host of other autoimmune diseases?
A 3-year, million dollar study of the VAERS system consigned to Harvard by HHS concluded that: "Adverse events from vaccines are common but underreported, with less than one percent reported to the Food and Drug Administration (FDA)."
Some available evidence suggests that vaccine deaths may be underreported by a factor of 20, but that's just conspicuous near-vaxx deaths and not later deaths from blood clot, stroke, heart failure, cancer, etc.
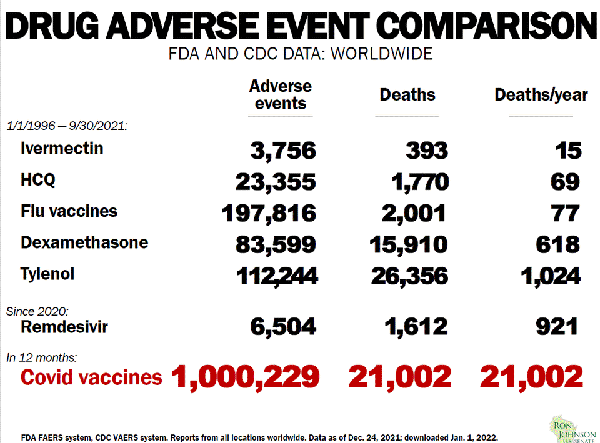
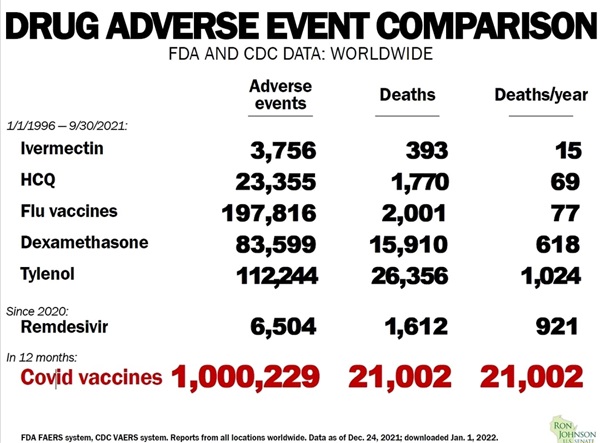
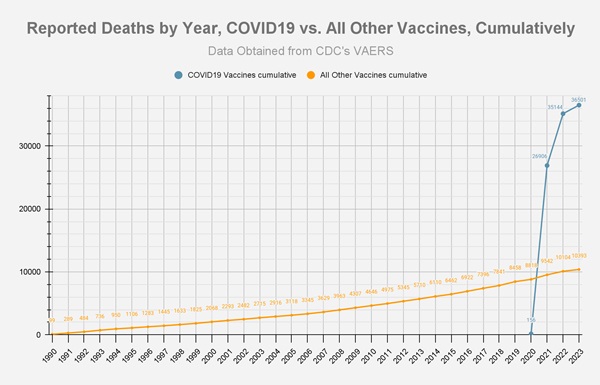
Even at the minimal rates reported to VAERS, the COVID vaccines have already chalked up over 3.5 times the deaths of all vaccines combined since 1990.
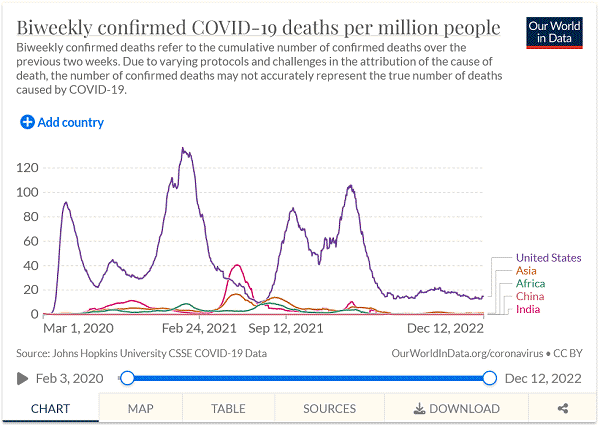
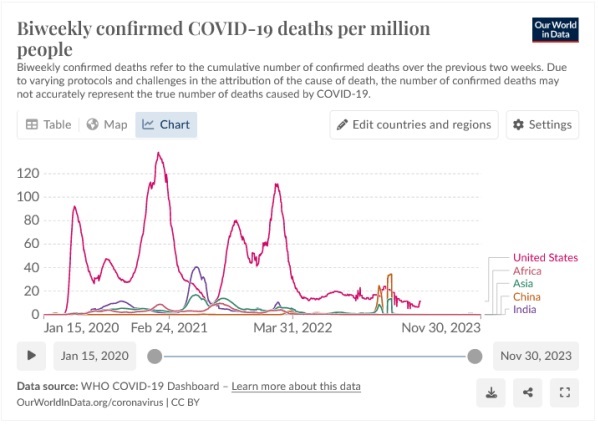
(link to here) The Case Fatality Rate makes the Big Pharma-captured West appear to be fairly average competitors in relative COVID treatment success. Is that because the U.S. had so many false positives that diluted the rate of deaths/cases because of high cycle thesholds (CTs) used in PCR testing artificially inflating the number of COVID cases, in order to gin up fear? Or perhaps for the 20% add-on to hospital Medicare reimbursement patients diagnosed as COVID positive?
Source of graph:
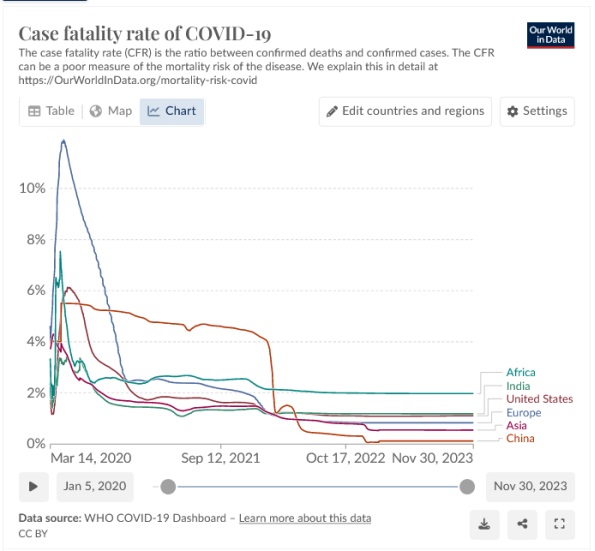
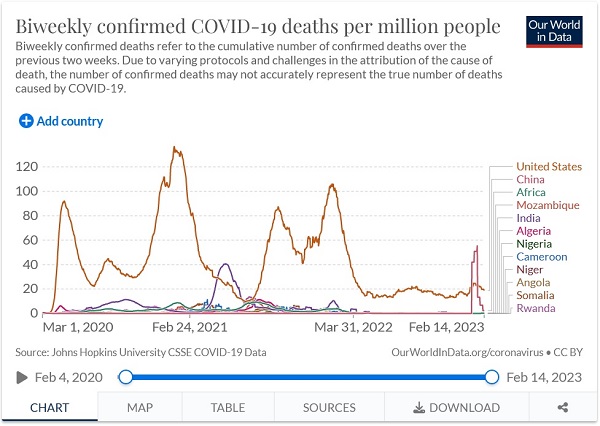
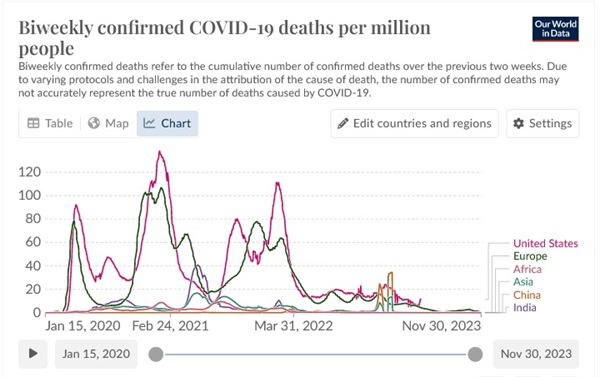
Does the following COVID death rate graph over the same period, confirm that the IVM and HCQ early treatment deprived West was other than a Big Pharma-driven COVID-19 killing field? Is that surprising when we consider that up to 99+% successful treatment of high-risk patients in the comfort of their own homes, since March of 2020 with $20 IVM & HCQ generic drug/nutraceutical protocols, was censored by Big Pharma's captured government and media in favor of their Illness Industry's Remdesivir and average $73,300 bill per hospital stay, in the U.S. corporatocracy?
The need for early treatment has been well known by competent clinicians since the beginning of the pandemic. For how many other illnesses do doctors deny early treatment until the patient becomes really sick? Why did Fauci suggest folks go home and isolate, with his NIH having no early treatment recommendations, until the individual began to suffocate from low oxygen and needed hospitalization? While doctors that were saving patients through the art and science of evidence-based medicine were forced to practice outside the NIH "Standard of Care", exposing them to increased liability exposure and license scrutiny. Doctors and nurses that spoke up in hospitals and other care facilities were fired or shunned, with the same for government workers and academics in Pharma-captured universities.
Blessedly it does appear as though the world is wising up.
So why are our kids being offered up as the dumping ground for unused product? Pharma's bureaucrats in our government even having included it on the childhood vaccine schedule, despite the known harms, for infants as young as 6 months old.
From 4 cases of myocarditis per million before COVID, to 25,000 cases per million.
And no, young people do not get myocarditis from COVID as much as they do from the experimental shots.
When Google/YouTube censors/bans the video in the following player you can access it at this BitChute link.
While the NIH continues to recommend against ivermectin outside of clinical trials, the Peruvian government approved the use of ivermectin by decree, on May 8 of 2020. Below left is a graph of the death rate of people over 60 years of age in 8 Peruvian states, before and after widespread distribution of ivermectin beginning on May 24th 2020, as compared to Lima (in red) which did not:
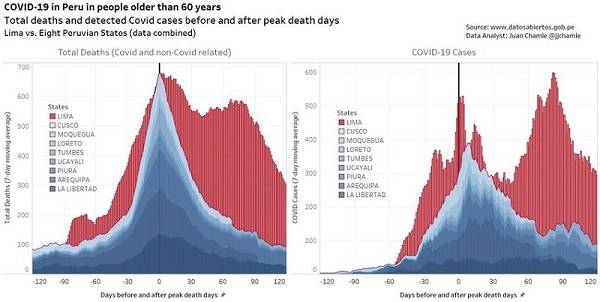
The above graph demonstrates how completely unnecessary it was to develop a vaccine, because ever since April of 2020 ivermectin has proven itself to be a highly effective treatment as well as pre-exposure prophylaxis for the SARS-CoV-2 virus, or as board-certified ICU critical care pulmonologist Dr. Pierre Kory put it while testifying before Congress: "If you are taking ivermectin you will not contract COVID-19".
In their continuing homicidal censorship, Google/YouTube censored Dr. Kory's congressional testimony in the player below, but fortunately it can still be accessed on BitChute at this link:
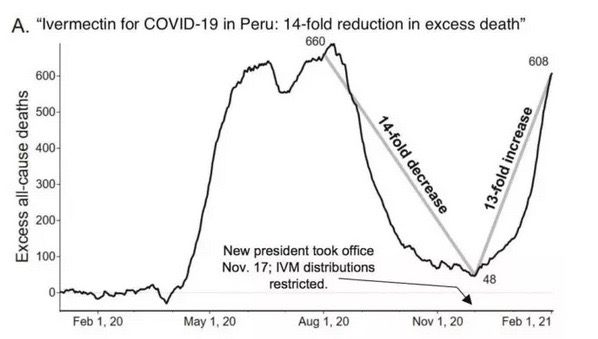
Update - Unfortunately, on Nov. 17th of 2020 Big Pharma and the bureaucrats they own prevailed in restricting ivermectin restricted in Peru and the graph demonstrates the tragic result. Same thing happened in India just as they were getting a handle on their surge that resulted from restrictions in ivermectin last year.
Below is an interview by Dr. Jennifer Hibberd, with three members of the Front Line COVID-19 Critical Care Alliance, on ivermectin. The ten doctors in the FLCCC have thousands of peer reviewed published papers and dozens of critical care books and chapters to their credit, that Big Pharma's journalist lackeys the NY Times unsurprisingly labeled as "quacks". Two members, Dr. Paul Marik and Dr. Peter McCollough, are the most published in their areas of expertise in world history, with Marik being the #2 most cited critical care doctor in the world. After Google/YouTube bans this video we will try to dig up a link at bitchute, rumble or brandnewtube.
The time to plan for COVID-19 infection is before you or your loved ones get sick. Formulate a plan of action now, that may include supplementing with vitamins and minerals to help prepare your system in advance of infection, as well as discussing or securing early treatment options. If you have been counting on your physician doing what's best for you after you get sick, the odds are better than not you will be treated the way over a million dead Americans were - who died completely unnecessary and horrific deaths from COVID-19 (at 4 to 100 times the rate of many of the poorest countries on earth) while some "long-haulers" may suffer for life - through what became the "standard of care". After investigating and deciding on an effective early treatment protocol, call your doctor and ask what early treatment protocol they prescribe for COVID-19, what symptoms their patients need to present in order to begin treatment, and at what point in the patient's disease progression they prescribe it. If your physician waits for results of notoriously unreliable PCR testing, before beginning treatment, find a more competent doctor.
Ivermectin has demonstrated itself to be up to 100% effective in early outpatient treatment of COVID-19, with a very impressive ability to rapidly reduce the viral load, dramatically reducing the period of time during which those that are infected are contagious. Ivermectin has even demonstrated its value in the hospitalized inpatient setting as well: "The blood oxygen level of the first patient treated in early April was 70%, and dropped to just 50% within hours. After receiving the invermectin, the patient stabilized within 24 hours and was discharged from the hospital in one week." For treatment it is prescribed along with doxycycline or azithromycin, and zinc, as well as vitamins and other supplements.
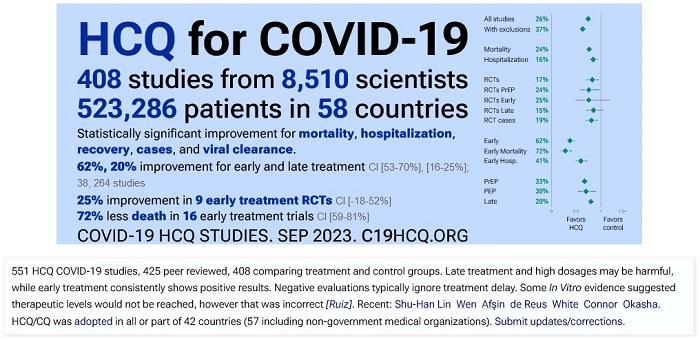
The world renowned Zelenko Protocol (or "COVID Cocktail") is another $20 COVID remedy that has been around since March of 2020, that employs hydroxychloroquine (HCQ) along with a zinc supplement and Azithromycin or doxycycline, that is effective in up to 100% of elderly or high-risk patients treated, when administered immediately upon the presentation of symptoms or clinical suspicion of COVID-19. Hydroxychloroquine has a 65-year record of safety that the AAPS suggests demonstrates it to be safer than aspirin, Tylenol or Benadryl. It is taken every day by millions of Americans - some over decades - for Lupus and rheumatoid arthritis, in the same dosage that the Zelenko Protocol prescribes over just seven days. It is available over the counter in many countries, as it was in France for over 50 years, as it should be here in the U.S.
Both of the above mentioned under $20 treatment protocols consist of pills that may be consumed at home, that are available and affordable around the world, and when taken on a timely basis are far superior in efficacy to expensive experimental new patented drugs. Intravenously administered $3,100-$5,700 Remdesivir/Veklury (Gilead's material cost perhaps under $10) for example, is impractical outside of a monitored hospital setting, has questionable efficacy, and may be associated with negative side effects on the kidneys, liver and heart, while the long term side effects are yet to be realized. On November 20th the WHO issued a conditional recommendation against the use of Remdesivir, then unsurprisingly just two days later the Big Pharma driven FDA did the exact opposite and formally approved it, even as the FDA continues to discourage the use of safe, proven, inexpensive 99+% effective hydroxychloroquine or ivermectin, as COVID remedies.
Again, if you are counting on your doctor to treat you as compassionately and competently as the doctors in the videos above, you are likely to be disappointed, so it's a good idea to inquire of your doctor ahead of time as well as plan and prepare for early treatment at home to reduce the odds of winding up in the hospital, particularly since FAIR Health suggests the average hospital bill stuck to a COVID-19 patient is around $73,300.
If you have been "vaccinated", as more recent stats suggest in terms of negative "vaccine" efficacy, preparing may be even more important for you.
Fatalities from COVID would likely be reduced by 90% or much more, if the U.S. health care community took the ethical and humane (but less profitable) approach of effective early outpatient treatment with cheap, generic, up to 100% effective, off-patent drugs whose safety has been established for 35 (ivermectin) and 65 (hydroxychloroquine) years. Indeed if we adopted an immediate national obsession of early treatment with proven protocols through public service announcements and such, we could theoretically reduce the number of COVID deaths by 95-100% within a few weeks and reach herd immunity rapidly, thereby reducing the opportunity for the virus to mutate further. There was never a PSA announcing that Americans should make sure their vitamin D levels were sufficient, since "Patients with Vit D deficiency were twice as likely to experience major complications".
So was it reasonable to rush injecting people with an unapproved, experimental, novel, biological/chemical agent, for one of the most treatable upper respiratory diseases to ever come along? What will the ultimate result of having done so be? For the full interview click here.
Doctors suggest that measures can be taken in advance of infection by the SARS-CoV-2 virus to better prepare our immune systems to inhibit its progression into COVID-19 disease. Zinc can equip our cells to more effectively inhibit viral replication, and supplementation is of particular importance for the elderly who tend to be zinc deficient (which should be taken along with a zinc ionophore like quercetin or hydroxychloroquine, plus vitamin C), while vitamin D deficiency is often associated with poor COVID outcomes. Researchers at Oregon State University estimate that 94% of people older than 4 in the United States have less-than-adequate levels of vitamin D. Some doctors suggest that ivermectin has demonstrated its value as a safe and effective prophylaxis for higher-risk individuals. One doctor went as far as to suggest that there is no such thing as a flu season, but rather a vitamin D deficiency season, because sunshine and resulting vitamin D levels become so low during the winter. In the case of COVID-19, an ounce of prevention is worth a ton of cure, and could even determine the difference between life and death. In other words, $20 worth of outpatient treatment, is worth $73,300 worth of iffy, dangerous and often insufficient, hospitalized "cure". There is a category in the forum dedicated to preparation and prevention at this link.
Compare treatment options and decide on your own preferences in advance of infection, then ask your doctor what course of action he would recommend and drugs he would prescribe, if you or your elderly loved ones were to become symptomatic. The last thing you need is to be let down by a CYA doctor's tepid "standard of care" treatment proposal, and wind up having to doctor shop after you or your loved one gets sick, because every day of delay reduces the chances of an anti-viral medication being its most effective. For this same reason, some doctors suggest it is ill-advised to wait for the result of an unreliable COVID test, before beginning treatment.
To "go home and isolate" is not a plan of action as much as a highway to hospitalization, while delays in treatment exponentially decrease the odds of survival, at least in the case of elderly or high-risk individuals. Even Tamiflu instructions say it needs to be taken within 2 days of the onset of symptoms. Humane physicians that are actually concerned about the welfare of their patients, model their care after competent clinicians like Dr. Zev Zelenko, Dr. Paul Marik of the I-MASK+ and MATH+ Protocols and likely most of the members of the AAPS. Dr. Brian Tyson treated 1,900 elderly and high-risk patients with the "COVID Cocktail" - as early as possible after the onset of symptoms or clinical suspicion of COVID-19 - and enjoyed an outcome of zero deaths and only one hospitalization of four days, over those 1,900 patients. More recent information suggests he has had similar success on over 2,500 patients.
The COVID-19 forum is a collection of video interviews and articles by treating physicians that detail their experiences in treating COVID-19 patients ever since February of 2020. There are also published works included, by and about world renowned microbiologists, virologists and epidemiologists, as well as studies that illustrate the effectiveness of various treatments. The information is presented to help the viewer decide on a personal plan of action and prepare their immune system in advance of infection to better cope with the SARS-CoV-2 virus, as well as to become familiar with treatments for COVID-19 that can best help their - particularly elderly or high-risk - loved ones.
Since we are not health care professionals nor scientists we do not offer treatment advice, however we do look forward to meeting with you in the forum and directing you toward information from those who are and do, that may help with any questions you develop. Additionally we are more than open to and indeed would very much appreciate, correction and constructive criticism, down to the smallest detail of this page or any post in the forum.
A PDF of this webpage is available at this link.
Please click this forum link for a few transcripts from the following very important video - "COVID-19: A Second Opinion - Senate testimony"
The video doesn't actually begin until the 40:19 minute mark.
Screenshots captured from "Select Treatment" link at https://c19early.org/
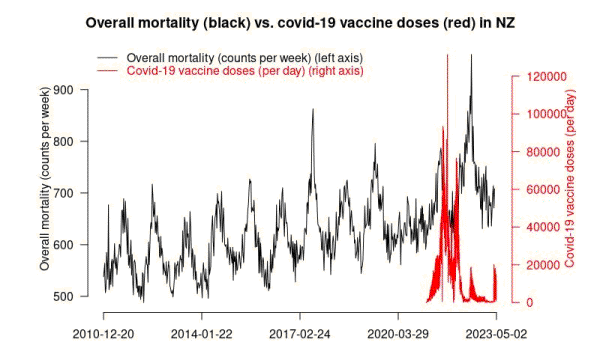
Following graph was sent to Steve Kirsh by a New Zealand scientist:
Older graphs, scroll up for more current..